Track your nutrition and health goals
Weight Loss Diet Plan for Women in India: Complete Guide

By Asfia Fatima, Chief Dietitian at Clearcals
Most generic weight-loss advice is written without accounting for how women's nutritional needs differ — menstrual cycle effects on appetite and water retention, higher iron and calcium requirements, and the specific safety considerations around pregnancy, breastfeeding, and PCOS. This guide addresses those gaps directly.
If you have been diagnosed with PCOD/PCOS specifically, see our dedicated PCOD diet chart for weight loss guide — this article covers general weight-loss nutrition for women without a specific hormonal diagnosis.
TL;DR
- Calorie needs: Most adult women lose weight sustainably at 1,400-1,800 kcal/day, depending on activity level and starting weight — very low-calorie diets (under 1,200 kcal) are not recommended without medical supervision
- Protein matters more than commonly assumed: Aim for 0.8-1.2g protein per kg body weight to preserve muscle during a deficit
- Iron and calcium are higher priorities for women, particularly those who menstruate, are postpartum, or are over 40
- Cycle-aware eating: Appetite and water retention naturally fluctuate through the menstrual cycle — this is normal, not a sign of "failure"
- Build and track a personalised plan with the Hint app
Calorie and Macronutrient Targets for Women
| Activity Level | Typical Calorie Range for Weight Loss |
|---|---|
| Sedentary (desk job, little exercise) | 1,400-1,600 kcal/day |
| Moderately active (light exercise 3-4x/week) | 1,600-1,800 kcal/day |
| Active (regular structured exercise) | 1,800-2,100 kcal/day |
These are general ranges — actual needs depend on current weight, height, age, and goals. A registered dietitian or a tool like Hint Pro can calculate a number specific to you rather than relying on a generic range.
Macronutrient guidance:
- Protein: 0.8-1.2g per kg body weight daily — supports satiety and preserves muscle mass during a deficit
- Fibre: 25-30g daily from vegetables, fruits, legumes, and whole grains
- Fat: Don't go below roughly 0.5-0.6g per kg body weight — very low fat intake can disrupt hormone production
- Iron: 18mg/day for menstruating women (higher than the 8mg/day typically recommended for men)
- Calcium: 1,000mg/day, rising to 1,200mg/day after age 50
Sample One-Day Indian Meal Plan (~1,600 kcal)
| Meal | Food | Approx. Calories |
|---|---|---|
| Breakfast | 2 vegetable-stuffed idlis + sambar, OR 1 bowl oats with milk and fruit | 250-300 kcal |
| Mid-morning | 1 medium fruit (apple/papaya/orange) | 60-90 kcal |
| Lunch | 2 rotis + 1 cup dal + 1 cup mixed vegetable curry + small salad | 450-500 kcal |
| Evening snack | 1 cup curd with roasted chana, OR a handful of nuts | 150-180 kcal |
| Dinner | 1 cup brown rice or 1-2 rotis + paneer/chicken/fish curry + sautéed greens | 450-500 kcal |
| Total | ~1,400-1,600 kcal |
Adjust portions up or down based on your calculated calorie target. This structure prioritises protein at each meal and fibre-rich vegetables, both important for satiety during a deficit.
Why Women's Weight Loss Needs Differ from Generic Advice
1. Menstrual Cycle Affects Appetite and Water Weight
In the luteal phase (roughly the two weeks before a period), many women experience increased appetite and water retention due to hormonal shifts (progesterone, oestrogen). A 1-2kg increase on the scale in this window is very commonly water retention, not fat gain — judging progress weekly rather than daily, and over the whole cycle, gives a clearer picture.
2. Iron Needs Are Higher
Menstruation causes regular iron loss. Combined with calorie restriction, this can increase the risk of iron-deficiency anaemia if the diet isn't planned carefully. Include iron-rich foods (dal, leafy greens, jaggery in moderation, lean meat/eggs) and pair plant-based iron sources with vitamin C (lemon, amla, citrus) to improve absorption.
3. Crash Diets Disrupt Hormones More in Women
Very low-calorie diets (under ~1,200 kcal/day) carry a higher risk of disrupting the menstrual cycle and thyroid function in women compared to a moderate, sustainable deficit. This is one of the clearest reasons "crash dieting" tends to backfire — both for hormonal health and for long-term weight maintenance.
4. PCOS and Insulin Resistance Are Common, Even Without Diagnosis
A significant share of Indian women have some degree of insulin resistance, with or without a formal PCOS diagnosis. A diet built around stable blood sugar — adequate protein and fibre at each meal, limiting refined carbohydrates — supports weight loss more effectively for these women than calorie counting alone.
5. Strength Training Is Particularly Underused
Women are statistically less likely than men to do resistance training, despite it being one of the most effective tools for preserving muscle (and a higher resting metabolism) during weight loss. See our guide on strength training for weight loss for how to start.
Special Situations
Postpartum: Weight loss after childbirth has its own pacing and safety considerations — see our dedicated postpartum weight loss guide rather than applying a standard deficit immediately after delivery, especially while breastfeeding.
PCOD/PCOS: Insulin-resistance-focused eating is especially important — see the PCOD diet chart for weight loss.
Perimenopause/Menopause: Metabolic rate and muscle mass naturally decline with hormonal changes around this life stage, often requiring a recalibrated calorie target and increased emphasis on strength training and protein.
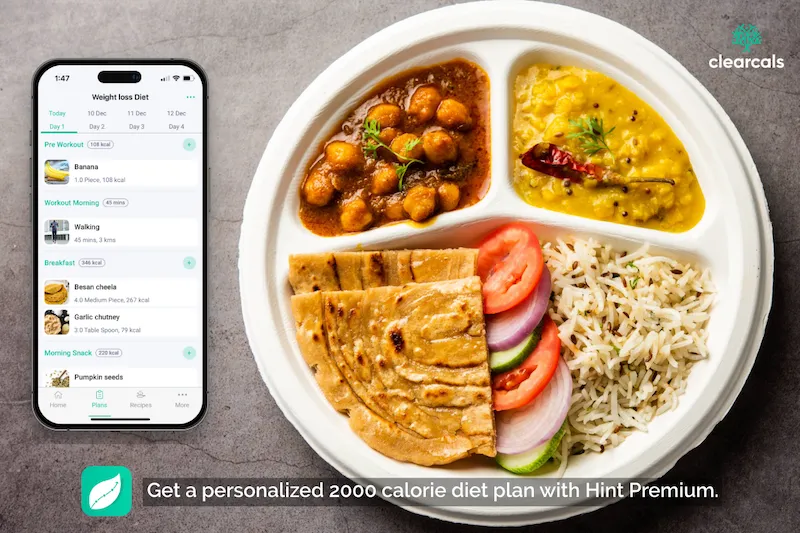
How the Hint App Supports Women's Weight Loss
The Hint app is built to account for exactly these factors:
- Personalised calorie and macro targets: Hint Pro calculates targets based on your specific profile, not a generic number
- Cycle-aware tracking: Log how you're feeling alongside your weight trend to separate water retention from real progress
- Indian food database: Track iron- and calcium-rich Indian foods accurately
- Dietitian consultations: Hint Premium connects you with a registered dietitian for a fully personalised plan, including for PCOS, postpartum, or perimenopausal needs
Frequently Asked Questions
How many calories should a woman eat per day to lose weight?
Most women lose weight sustainably between 1,400-1,800 kcal/day, depending on activity level, height, and starting weight. Going below ~1,200 kcal/day without medical supervision is generally not recommended.
Why does my weight fluctuate so much during the month?
Hormonal shifts across the menstrual cycle cause real water retention, particularly in the week or two before your period. This is normal and not necessarily related to fat gain or loss — track trends over weeks, not single days.
Is intermittent fasting safe for women?
It can be, but women may be more sensitive to extended fasting windows than men, particularly with respect to hormonal balance. Start with a moderate window (such as 12-14 hours) and monitor your cycle and energy levels; see our intermittent fasting guide for more detail.
Should women avoid weights/strength training while trying to lose weight?
No — strength training helps preserve muscle mass during a calorie deficit and does not cause women to "bulk up" without a substantial calorie surplus. It is one of the most underused tools for sustainable weight loss in women.
Is it harder for women to lose weight than men?
Women generally have a higher percentage of body fat and a lower muscle mass at the same body weight as men, which can mean a somewhat lower calorie burn at rest. This is a real biological difference, but it does not make weight loss impossible — it means calorie targets and expectations should be calibrated accordingly.
What should I eat for weight loss during my period?
Continue your normal balanced diet; iron-rich foods (dal, leafy greens, lean protein) are particularly useful during menstruation. Cravings are common — a controlled portion of a craved food is more sustainable than total restriction.
References
- ICMR-National Institute of Nutrition. Nutrient Requirements for Indians — Recommended Dietary Allowances (RDA), 2020.
- Reed BG, Carr BR. The Normal Menstrual Cycle and the Control of Ovulation. Endotext. StatPearls/NCBI.
- Westerterp-Plantenga MS. Protein intake and energy balance. Regul Pept. 2008;149(1-3):67-9. DOI: 10.1016/j.regpep.2007.08.026
Explore More
- PCOD Diet Chart for Weight Loss
- The Benefits of Strength Training for Weight Loss
- Weight Loss Diet Plan — India
- Postpartum Weight Loss
About the Author
Asfia Fatima is the Chief Dietitian at Clearcals, with a Master's Degree in Dietetics and Clinical Nutrition and over a decade of experience in clinical nutrition and lifestyle management.
She specialises in evidence-based diet planning for weight loss, diabetes, and metabolic health. At Clearcals, she leads the nutrition strategy behind the Hint app, helping users achieve their goals with science-backed guidance.
🔗 Connect with Asfia on LinkedIn