Track your nutrition and health goals
Low HRV: Causes, Symptoms, What It Means and What to Do
By Dr. Krishna Athmakuri, Cofounder & CEO, Clearcals | Updated: May 2026
What Does Low HRV Actually Mean?
Heart rate variability measures the variation in time between consecutive heartbeats.
A high HRV indicates that the heart is responding fluidly to autonomic nervous system signals — the beat-to-beat interval is constantly adjusting to meet physiological demand.
A low HRV indicates the opposite: the heart is beating with less flexibility, with intervals that are more rigid and uniform. This reduced variability reflects impaired autonomic regulation, specifically a reduction in parasympathetic (vagal) tone relative to sympathetic activity.
Low HRV is not a diagnosis in itself, but it is a reliable signal that something is suppressing your body's restorative, recovery-oriented nervous system function.
In clinical cardiology, persistently low HRV in patients with prior heart attack is one of the strongest independent predictors of mortality.
In otherwise healthy people, chronically low HRV is associated with insulin resistance, systemic inflammation, poor sleep quality, and increased all-cause mortality risk — even in the absence of overt disease.
The key distinction is between acutely low HRV (temporarily below your personal baseline due to a specific stressor) and chronically low HRV (persistently below population norms for your age group over weeks to months). The former is normal and expected. The latter warrants investigation.
What Is Considered Low HRV by Age?
"Low" HRV is defined relative to two standards: your personal established baseline, and population reference ranges for your age group.
Using RMSSD (the metric reported by Garmin, WHOOP, and Oura Ring), the following values represent the "Low" threshold — readings that fall below these levels for your age group over several consecutive weeks are clinically meaningful:
| Age Group | Low HRV Threshold (RMSSD, ms) |
|---|---|
| 18–25 years | Below 35 ms |
| 26–35 years | Below 30 ms |
| 36–45 years | Below 25 ms |
| 46–55 years | Below 20 ms |
| 56–65 years | Below 16 ms |
| Above 65 years | Below 12 ms |
Note on Apple Watch users: Apple Watch reports SDNN, not RMSSD. SDNN values are typically 30–50% higher than RMSSD in the same person. The thresholds above apply to RMSSD readings only and cannot be applied to Apple Watch Health app figures.
A single low reading is meaningless — one poor night's sleep, an evening of alcohol, or intense exercise the previous day can all suppress overnight HRV significantly.
Low HRV becomes medically relevant when it is persistent: consistently below your personal baseline for 5 or more consecutive days, or below the age-adjusted threshold above when measured over a 2–3 week period.
What Is Dangerously Low HRV?
This is one of the most-searched questions about HRV, and it deserves a careful, honest answer.
In clinical cardiology, a 24-hour SDNN below 50ms in post-myocardial infarction patients is strongly associated with increased mortality risk. This is a well-validated clinical threshold, but it applies to a specific patient population, uses a specific measurement method (24-hour Holter recording), and represents a different context from consumer wearable monitoring.
For healthy individuals tracking HRV on a wearable device, there is no universally agreed "dangerous" RMSSD threshold. However, the following patterns warrant medical evaluation:
- RMSSD consistently below the "Low" threshold for your age group over 3+ weeks with no identifiable lifestyle cause
- RMSSD falling more than 25–30% below your personal established baseline and staying there
- Low HRV accompanied by new symptoms: palpitations, unexplained fatigue, chest discomfort, significant sleep disruption, or rapid unexplained weight change
- Progressive decline in HRV over months without a corresponding change in lifestyle factors
If any of the above apply, the HRV reading itself is not the emergency, but it may be indicating an underlying condition that warrants investigation. A physician evaluation, including fasting metabolic panel, thyroid function, and blood pressure assessment, is a reasonable starting point.
Common Causes of Low HRV
1. Poor Sleep Quality and Chronic Sleep Restriction
Sleep is the primary restorative window for the parasympathetic nervous system. HRV is highest during deep sleep (slow-wave sleep), when vagal tone reaches its peak.
Chronic sleep restriction — even modest reductions to 6 hours per night — significantly impairs this parasympathetic restoration, producing persistently low baseline HRV.
Obstructive sleep apnoea is a particularly potent HRV suppressor: the repeated arousals and hypoxic episodes drive sustained sympathetic activation that carries over into waking hours.
2. Insulin Resistance and Metabolic Dysfunction
Insulin resistance impairs HRV through multiple mechanisms. Elevated insulin and blood glucose directly reduce vagal tone via effects on central autonomic nuclei.
Accumulating visceral fat produces chronic low-grade inflammation (through adipokine secretion) that further suppresses parasympathetic function.
Cross-sectional studies consistently show that people with metabolic syndrome have significantly lower HRV than metabolically healthy individuals of the same age, and that the degree of insulin resistance predicts the degree of HRV impairment.
3. Chronic Psychological Stress
The hypothalamic-pituitary-adrenal (HPA) axis and the autonomic nervous system are tightly coupled. Chronic psychological stress maintains elevated cortisol, which promotes sympathetic dominance and reduces vagal tone.
This is the physiological mechanism behind what people subjectively describe as feeling "wired but tired" — the autonomic system is locked in a sympathetically-driven, low-variability state even during rest.
The suppression is not merely psychological: HRV measurements objectively confirm reduced parasympathetic tone in individuals with chronic work stress, burnout, and anxiety disorders.
4. Overtraining and Insufficient Recovery
Exercise is the most powerful chronic HRV improver — but acute hard exercise temporarily suppresses HRV. This is normal and expected. The problem arises when training load consistently exceeds the body's recovery capacity.
In overtraining syndrome, the autonomic nervous system cannot return to baseline between sessions, producing a sustained low-HRV state that resembles — and is physiologically similar to — chronic psychological stress.
Athletes monitoring HRV as a training guide use persistent multi-day HRV suppression below baseline as the primary indicator that additional loading should not be applied.
5. Cardiovascular Risk Factors
Hypertension, dyslipidemia, and smoking each independently reduce HRV.
The mechanisms overlap: endothelial dysfunction, reduced arterial compliance, elevated sympathetic outflow, and structural cardiac changes all contribute.
In hypertensive individuals, the degree of HRV impairment correlates with the degree of blood pressure elevation and left ventricular hypertrophy — reflecting the cumulative autonomic cost of maintained elevated pressure.
6. Thyroid Dysfunction
Both hypothyroidism and hyperthyroidism alter autonomic balance and suppress HRV through different mechanisms.
Hypothyroidism reduces overall cardiac autonomic modulation and is associated with reduced RMSSD. Hyperthyroidism drives sympathetic dominance and tachycardia, reducing the absolute variability available.
Thyroid function is frequently overlooked in HRV assessment but should be evaluated when HRV is persistently low without an obvious lifestyle explanation — particularly in women, in whom thyroid dysfunction is substantially more common.
7. Alcohol Consumption
Alcohol is one of the most consistent, measurable acute HRV suppressors. Even moderate consumption (1–2 standard drinks) produces a measurable reduction in overnight HRV of 15–25%.
With heavier consumption, the effect is larger and persists for up to 72 hours.
Chronic alcohol use produces sustained HRV impairment through direct vagal nerve damage, liver-mediated metabolic dysfunction, and disruption of sleep architecture.
8. Obesity and Visceral Adiposity
Excess visceral fat independently suppresses HRV through adipokine-mediated inflammation, mechanical restriction of cardiac function, and the accompanying metabolic burden of insulin resistance and dyslipidaemia.
Weight loss studies consistently demonstrate HRV improvement proportional to fat mass reduction — even when the weight loss is achieved through caloric restriction alone, confirming that the fat mass itself (not merely the exercise used to lose it) contributes to HRV suppression.
9. Medications
Several commonly prescribed medications alter HRV. Beta-blockers reduce heart rate and HRV (this is pharmacologically intended in their cardiac indications).
SSRIs and SNRIs used for depression and anxiety have mixed effects — some studies show HRV improvement with effective treatment of the underlying condition, others show direct pharmacological reduction in HRV.
ACE inhibitors and statins may modestly improve HRV as a secondary effect of their primary cardiovascular actions.
Low HRV Symptoms: What You Might Notice
Low HRV itself is not a symptom-producing condition — it is a measurable signal of autonomic imbalance. However, the physiological state that causes low HRV often produces recognisable symptoms:
Fatigue and poor recovery: Persistent tiredness that does not resolve with sleep, feeling unrefreshed in the morning, slow recovery after exercise, and reduced physical performance are consistent features of the chronic low-HRV state.
Sleep disturbances: Difficulty falling asleep, frequent night waking, light or non-restorative sleep — these both cause and result from HRV suppression, creating a bidirectional cycle.
Mood changes: Heightened anxiety, irritability, emotional reactivity, and low stress tolerance often accompany low HRV states, reflecting the same sympathetic dominance that suppresses parasympathetic function.
Reduced heart rate variability during the day: If you notice your heart rate remains elevated even at rest, or fluctuates less than it used to during quiet periods, this may be a direct manifestation of reduced autonomic tone.
Elevated resting heart rate: Low HRV and elevated resting heart rate frequently co-occur, both reflecting the same sympathetic-dominant autonomic state.
It is important to note that these symptoms have many potential causes. Low HRV data adds an objective, measurable dimension to subjective symptoms — it does not replace clinical evaluation when symptoms are significant.
What to Do About Low HRV
Short-term (acute low HRV):
When your HRV drops acutely below your baseline, the appropriate response depends on the likely cause. If the previous day included hard training, high alcohol intake, very poor sleep, or known psychological stress, the cause is identified, and the response is straightforward: reduce training load, prioritise sleep, and avoid alcohol. The HRV typically returns toward baseline within 1–3 days.
Garmin's Low and Poor HRV Status categories are specifically designed to guide training response: reduce intensity to 30–50% of normal on Low days, and to light activity only on Poor days.
Long-term (chronically low HRV):
Chronic HRV improvement requires addressing the underlying cause. The evidence-based interventions with the strongest effect sizes are:
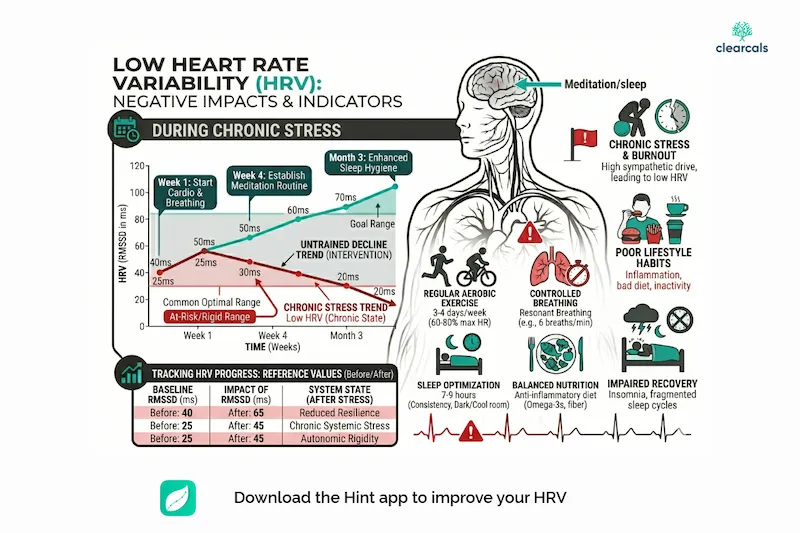
Aerobic exercise: Progressive aerobic training is the most potent chronic HRV intervention, with effect sizes comparable to pharmacological autonomic modulation. 30–45 minutes of moderate-intensity aerobic exercise, 4–5 times per week, produces measurable HRV improvement within 6–8 weeks and continues to improve HRV over months to years.
Sleep quality improvement: Addressing sleep hygiene, treating obstructive sleep apnoea, and maintaining consistent sleep timing all produce meaningful HRV improvement by restoring parasympathetic dominance during sleep.
Weight and metabolic improvement: In overweight individuals, caloric deficit that produces fat mass reduction improves HRV — this is true even without exercise, confirming the independent contribution of visceral adiposity.
Stress management: Structured stress reduction practices — particularly resonance frequency breathing (slow, paced breathing at approximately 6 breaths per minute) — have robust evidence for HRV improvement, with several randomised trials demonstrating effect sizes comparable to pharmacological parasympathomimetic drugs.
Addressing underlying medical conditions: Treating hypertension, optimising thyroid function, and managing insulin resistance each produce HRV improvement as a secondary benefit of metabolic normalisation.
A detailed breakdown of these interventions with protocols and expected timelines is available in How to Improve HRV.
When to See a Doctor About Low HRV
Low HRV on a consumer wearable is not itself a medical emergency, but it can be an early warning signal worth acting on. Consider consulting a physician if:
- HRV has been persistently below the "Low" threshold for your age group for more than 3–4 weeks
- The decline is accompanied by new or worsening symptoms (unexplained fatigue, palpitations, chest discomfort, significant weight change, sleep disruption)
- You have known cardiovascular risk factors (diabetes, hypertension, family history of heart disease), and your HRV is declining
- Your HRV dropped suddenly (more than 30% below baseline) without any identifiable lifestyle cause, and has not recovered
- You are concerned
A reasonable initial evaluation includes fasting blood glucose and insulin, HbA1c, thyroid function tests, full lipid panel, blood pressure, and a brief sleep history. Most causes of persistently low HRV are identifiable and addressable through this basic workup.
References
- Bigger JT, et al. Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation. 1992;85(1):164–171.
- Carnethon MR, et al. Associations among autonomic nervous system function, sleep quality, and HRV. Diabetes Care. 2003;26(7):1960–1966.
- Thayer JF, et al. A meta-analysis of heart rate variability and neuroimaging studies: implications for heart rate variability as a marker of stress and health. Neuroscience & Biobehavioral Reviews. 2012;36(2):747–756.
- Stein PK, et al. Traditional and nonlinear heart rate variability are each independently associated with mortality after myocardial infarction. Journal of Cardiovascular Electrophysiology. 2005;16(1):13–20.
- Ingjaldsson JT, et al. Reduced heart rate variability in chronic alcohol abuse: relationship with negative mood, chronic thought suppression, and compulsive drinking. Biological Psychiatry. 2003;54(12):1427–1436.
About the Author
Dr. Krishna Athmakuri is the Co-Founder and CEO of Clearcals, where he leads the development of data-driven health technology through the Hint app.
With a Ph.D. in Chemical Engineering from Rensselaer Polytechnic Institute, New York, his expertise spans analytics, protein chemistry, and biotechnology.
Earlier in his career, he developed biotherapeutics for diabetes and metabolic diseases at companies like Aurobindo Pharma and Dr. Reddy's Laboratories.
At Clearcals, he now applies that scientific rigour to build personalised fitness tools — including Hint Pro Workouts, nutrition tracking, and real-time metabolic insights — helping users make smarter health decisions through technology.
Connect with Dr. Krishna on LinkedIn
👉 Back to the pillar page: Heart Rate Variability (HRV): Complete Guide 👉 Related: HRV Normal Range by Age | How to Improve HRV | HRV and Sleep